Pre operation
Ten days prior to the procedure you should:
- Have your blood and urine test
- Notify Mr Thyer’s rooms if you are taking any blood thinning medication
The procedure
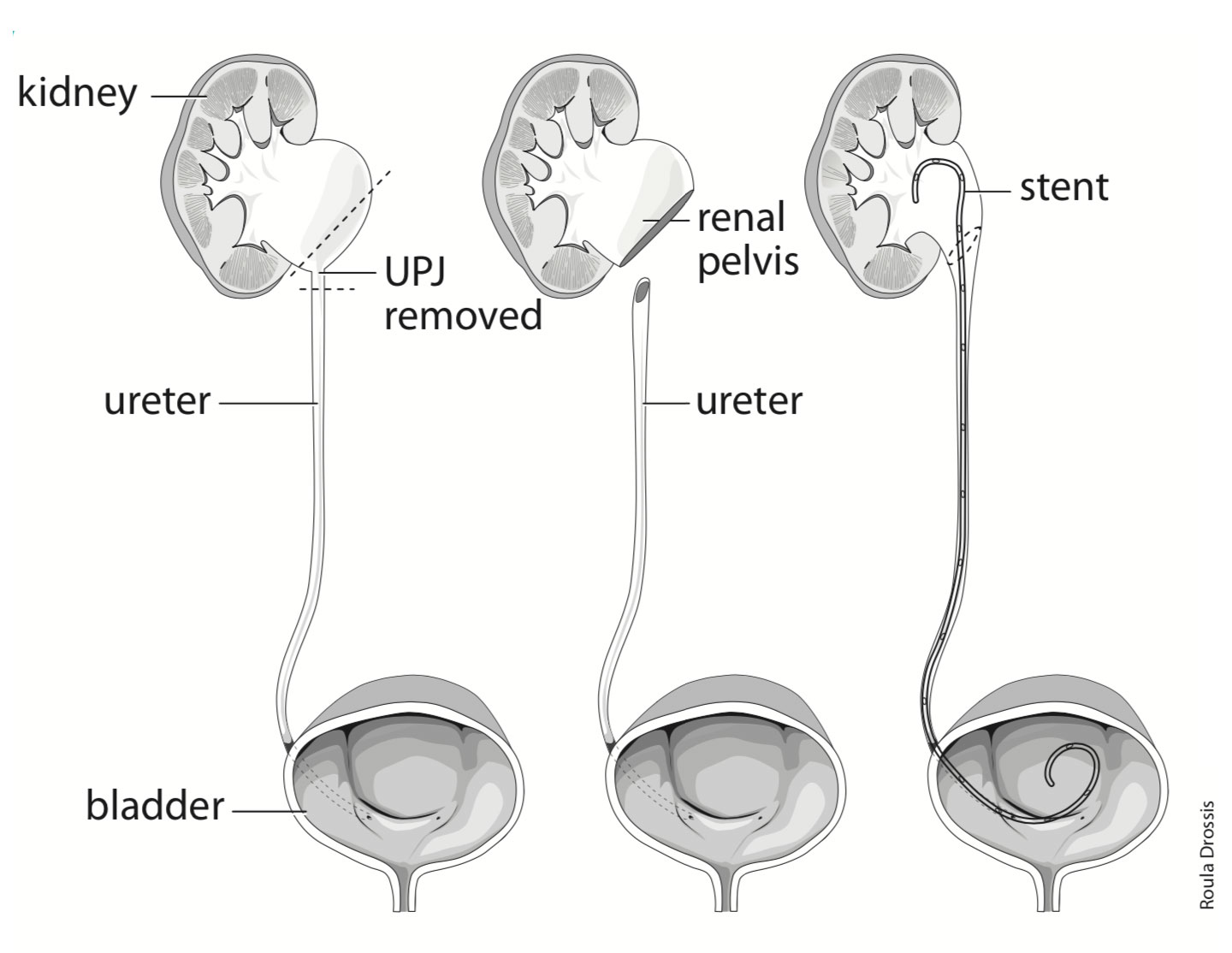
On arrival at hospital you will be prepared for theatre by nursing staff. Mr Thyer will see you just prior to being taken into the operating theatre. You will require a general anaesthetic of approximately 1.5 hours. Mr Thyer will make a series of 3-4 small incisions in the abdomen to allow the passage of the laparoscopic instruments. The PUJ will be dissected free from the surrounding structures, the narrowed section removed then the ureter will be sutured back on to the renal pelvis so that the narrowing is no longer present. The PUJ may be sent to a pathologist for microscopic examination (you may incur a pathologist fee). A stent will be left in place within the ureter to act as a splint whilst the new PUJ heals. After the operation a small drain will be left in the abdomen and a catheter in the bladder. Most people are in hospital 1-2 nights then discharged home after Mr Thyer’s review.